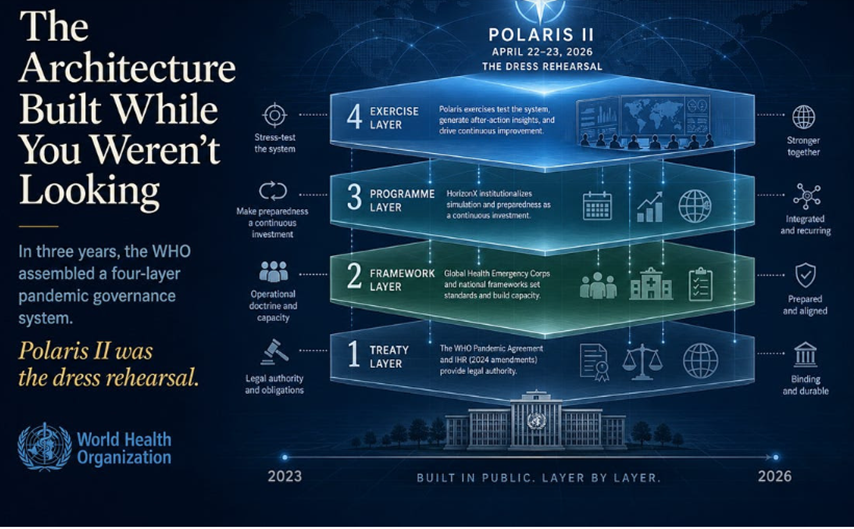
Kolmessa vuodessa WHO on koonnut nelikerroksisen pandemianhallintajärjestelmän. Polaris II oli kenraaliharjoitus.
Alempana on käännös Tri Robert W. Malonen kirjoituksesta. Haluan korostaa, etteivät tulkinnat ole minun. Käytin Google translate -työkalua tekstiä kääntäessäni. Käännöstä on luettu ja ilmaisut on tarkistettu selkeyden vuoksi. Tekstin lihavointi on minun.
Tamara Tuuminen, erikoislääkäri, dosentti
Samalla kun poliittinen luokka on viimeiset kolme vuotta väitellyt siitä, yrittikö Maailman terveysjärjestö (WHO) salaa vallata maailman, WHO on tehnyt jotain paljon mielenkiintoisempaa ja merkittävämpää. Se rakensi kaikkien silmien alla kattavan arkkitehtuurin seuraavan pandemian hallitsemiseksi. Ja sitten se piti kenraaliharjoituksen.
Kenraaliharjoituksen nimi oli Harjoitus Polaris II. Se järjestettiin 22.-23.4. 2026. Harjoitukseen osallistui 26 maata, 600 terveysalan hätätilanteiden asiantuntijaa ja yli 25 kumppaniorganisaatiota. Skenaario oli kuvitteellinen uusi bakteeri, joka oli levinnyt 27 maahan ja julistettu kansainväliseksi kansanterveydelliseksi hätätilaksi (1). Maat aktivoivat hätätilanteiden koordinointirakenteensa, mobilisoivat työvoimaa, yhdenmukaistivat käytäntöjä rajojen yli ja (tässä kannattaa pysähtyä), tutkivat tekoälypohjaisia työkaluja työvoiman suunnitteluun. (2)
Jos lukee vain lehdistötiedotteen, niin tämä näyttää pöytäharjoitukselta. ”Kuivaharjoittelulta”. Hyödylliseltä jopa, kun otetaan huomioon, että edellinen pandemia tappoi miljoonia ja paljasti todellisia koordinointiongelmia. Kuka voisi vastustaa harjoittelua?
Polaris II ei kuitenkaan ole erillinen tapahtuma. Se on näkyvä osa jotain paljon laajempaa kokonaisuutta, jota on rakennettu pala palalta vuodesta 2023 lähtien. Ja kun rakenteen kerran huomaa, sitä on vaikea enää olla huomaamatta.
Neljä kerrosta, kolme vuotta
Se, mitä on itse asiassa rakennettu, on tiiviisti toisiinsa kytkeytyvä, nelikerroksinen järjestelmä, joka on kehittynyt huomattavan nopeasti:
Kerros 1: Sopimuskerros. Maailman terveysjärjestön 78. kokous hyväksyi 20. toukokuuta 2025 WHO:n pandemiasopimuksen äänin 124 puolesta, 0 vastaan ja 11 tyhjää (3). Se on vasta toinen oikeudellisesti sitova sopimus, joka on koskaan neuvoteltu WHO:n peruskirjan 19 artiklan nojalla. (4) Ensimmäinen oli vuoden 2003 tupakoinnin torjuntaa koskeva puitesopimus, ja useimmat ihmiset eivät ole koskaan kuulleet siitä, koska tupakka on epäsuosittua ja sopimus oli kiistaton. Tämä on erilainen. Pandemiasopimus perustaa taudinaiheuttajien saatavuuden ja hyötyjen jakojärjestelmän, maailmanlaajuisen toimitusketjun ja logistiikkaverkoston sekä uuden rahoitusmekanismin. (5) Se tulee voimaan 30 päivää sen jälkeen, kun 60 valtiota on ratifioinut sen, ja kun parhaillaan vuoden 2026 aikana neuvoteltava PABS-liite on saatettu valmiiksi. (6)
Sopimuksen rinnalla ovat vuoden 2024 muutokset kansainvälisiin terveyssääntöihin, jotka tulivat voimaan syyskuussa 2025. Muiden muutosten ohella otettiin käyttöön uusi ”pandemian hätätila” -hälytystaso, joka on yksi taso korkeampi kuin nykyinen kansainvälisesti merkittävän kansanterveyshätätilan luokitus. (7) Kansainvälinen terveyssäännöstö on sitonut jäsenvaltioita vuodesta 2005 lähtien. Muutokset laajentavat sen operatiivista ulottuvuutta.
Kerros 2: Kehyskerros. Maailman terveyshätäapuryhmä (tai -verkosto) (Global Health Emergency Corps, GHEC) perustettiin toukokuussa 2023 pidetyssä Maailman terveyskokouksessa. (8) Sen omassa puiteasiakirjassa sitä kuvaillaan ”enemmän kuin työvoimakehykseksi; se on sitoutuminen globaaliin solidaarisuuteen, jossa priorisoidaan itsemääräämisoikeutta ja oikeudenmukaisuutta”. (9) Käytännössä kyseessä on pysyvä, maailmanlaajuinen kansallisten hätäapuryhmien verkosto, johon kuuluu mekanismeja rajat ylittävään lisävoimien lähettämiseen. Verkosto otettiin ensimmäisen kerran käyttöön lokakuussa 2024 vastauksena Kongon demokraattisessa tasavallassa puhjenneeseen mpox-epidemiaan. (10)
Lokakuussa 2025 WHO julkaisi kansallisen terveyshätätilan hälytys- ja reagointikehyksen (11). Tässä asiakirjassa kerrotaan maille, miten niiden tulisi jäsentää kotimaiset hätätilanteisiin reagointinsa: havaitseminen, ilmoittaminen, riskinarviointi, aktivointi, interventio, jälkitarkastelu. Se sisältää 7-1-7-suorituskykytavoitteen: seitsemän päivää epidemian havaitsemiseen, yksi päivä viranomaisille ilmoittamiseen ja seitsemän päivää varhaisten toimien toteuttamiseen. (12) Se yhdistää yli 300 COVID-19 -arvioinneista saatua suositusta yhdeksi kansalliseksi doktriiniksi. (13)
Kerros 3: Ohjelmakerros. HorizonX on kattava ohjelma, joka muuttaa simulaatioharjoitukset kertaluonteisista tapahtumista pysyväksi, toistuvaksi testijärjestelmäksi. Se käynnistettiin lokakuussa 2024 monivuotisena hankkeena, jonka tavoitteena on ”monialainen varautuminen eläimistä ihmisiin tarttuvien sairauksien hätätilanteisiin”. (14) Polaris on vain yksi osa-alue. WHO järjesti noin 50 simulaatioharjoitusta pelkästään vuonna 2025. (15) WHO:n omissa materiaaleissa käytetty ilmaisu on paljastava: varautumisen on tarkoitus olla ”jatkuva investointi” eikä ”ajoittaista toimintaa”. (16)
Kerros 4: Harjoituskerros. Polaris I huhtikuussa 2025, mukana yli 15 maata. (17) Polaris II huhtikuussa 2026, mukana 26 maata. (1) Harjoitusten on suunniteltu jatkuvan HorizonX:n alaisuudessa toistaiseksi. Jokainen harjoitus testaa sen yläpuolella olevia kerroksia ja tuottaa jälkiarviointiraportin, jota hyödynnetään järjestelmän kehittämisessä. (18)
Tämä ei ole byrokratian sattumaa. Kyseessä on tarkoituksellisesti suunniteltu järjestelmä. Jokainen taso tukee seuraavaa. Sopimus tarjoaa oikeudellisen perustan. Toimintakehykset määrittelevät toimintaperiaatteet. Ohjelma vakiinnuttaa käytännöt. Harjoitukset tuottavat empiirisen perustelun järjestelmän laajentamiselle.
MITÄ WHO TÄSTÄ SANOO
WHO ei salaile mitään tästä. Pääjohtaja sanoi sen suoraan Polaris II -harjoituksen päätyttyä: ”Polaris II -harjoitus osoitti, mikä on mahdollista, kun toimimme yhdessä. Se osoitti, että globaali yhteistyö ei ole valinnaista; se on välttämätöntä”. (19)
Lue tuo lause uudelleen. Ei valinnaista.
Tämä ei ole tasa-arvoisten suvereenien valtioiden välisen vapaaehtoisen kansainvälisen yhteistyön kieltä. Se on moraalisen velvoitteen kieltä, jota tukee institutionaalinen arkkitehtuuri. Pääjohtaja sanoo (hänen näkökulmastaan oikein), että WHO on käyttänyt kolme vuotta rakentaen järjestelmää, jossa yhteistyöstä kieltäytyminen ei ole enää vakava vaihtoehto millekään maalle, joka haluaa pysyä osana globaalia terveysjärjestystä.
Vertaisarvioitu artikkeli National Library of Medicine -tietokannassa tekee kerrosten välisen yhteyden selväksi. Siinä todetaan, että pandemiasopimus ”vahvistaa GHEC:n (kansallisten hätäapuryhmien) merkitystä korostamalla, että jokaisen maan tulisi ’kehittää, vahvistaa ja suojella ammattitaitoista ja riittävää työvoimaa terveyskriisien ehkäisemiseksi, niihin varautumiseksi ja reagoimiseksi, myös pandemioiden aikana’.” Artikkelissa jatketaan: ”Globaalit hätäapuryhmät, joilla on nopean toiminnan ja kansainvälisen terveysasiantuntemuksen mandaatti, toimivat sopimuksen operatiivisena osana. Se muuttaa sopimuksen korkean tason sitoumukset toiminnaksi”. (20)
Tässä ei ole epäselvyyttä. Kehys on sopimuksen operatiivinen osa. Harjoitus testaa kehystä. Ohjelma tekee testauksesta pysyvää. Sopimus tekee koko asiasta oikeudellisesti kestävän.
SUVERENITEETTIKYSYMYS REHELLISESTI SANOTTUNA
Vallitsevan vallan tavanomainen vastaus tätä arkkitehtuuria koskeviin huolenaiheisiin on osoittaa tiettyihin lausekkeisiin ja sanoa: katso, sopimus säilyttää suvereniteetin. Tekstissä todetaan nimenomaisesti, ettei se valtuuta WHO:ta ohjaamaan, määräämään tai muuttamaan kansallisia lakeja. Ison-Britannian ministerit ovat todenneet, ettei WHO:lla ole missään olosuhteissa valtaa määrätä sulkutoimia. (21) WHO:n tiedottajat hylkäävät suvereniteettihuolet vääränä tietona.
Nämä lausunnot ovat teknisesti tarkkoja. Ne ovat myös hieman asian vierestä.
Nykyaikaisessa hallintovaltiossa suvereniteetista luovutaan harvoin yhdellä dramaattisella teolla. Se rapistuu vähitellen pehmeiden sitoumusten, teknisten standardien, suorituskykyvertailuarvojen, vertaispaineen, rahoitusehtojen ja informaatioriippuvuuksien kasautumisen myötä. Maa, joka on allekirjoittanut pandemiasopimuksen, uudistanut kansallisen hätätilanteiden henkilöstönsä ohjeiden mukaisesti, ottanut käyttöön kansallisen hälytys- ja reagointikehyksen 7-1-7 -aikataulut, integroinut valvontansa maailmanlaajuiseen epidemian hälytys- ja reagointiverkostoon ja sitoutunut osallistumaan HorizonX-harjoituksiin, ei ole virallisesti luopunut mistään suvereniteetista. Se on vain tehnyt kymmeniä käytännön valintoja, jotka kokonaisuutena tarkasteltuna tarkoittavat, että sen pandemian torjunta on toiminnallisesti erottamaton siitä, mitä WHO olisi määrännyt.
Tämä ei ole salaliitto. Se on normaali mekanismi, jolla kansainväliset teknokraattiset järjestelmät toimivat. Euroopan unioni toimii näin. Kansainvälinen valuuttarahasto IMF toimii näin. OECD toimii näin. Uutta on WHO:n mallin nopeus ja laajuus sekä se, että se on rakennettu nimenomaan hätävaltuuksien ympärille, alalle, jossa kansalaiset ovat perinteisesti osoittaneet valtavaa kunnioitusta sille taholle, joka on määritelty lailliseksi auktoriteetiksi.
Kun seuraava taudinaiheuttaja ilmestyy, kysymys ei ole siitä, säilyttävätkö kansalliset hallitukset laillisen oikeuden päättää omasta toimintatavastaan. Ne säilyttävät sen. Kysymys on siitä, onko millään hallituksella poliittisesti mahdollista poiketa linjasta hätätilanteen kuumimmassa vaiheessa, kun sen omat instituutiot on integroitu WHO:n toimintakehyksiin, sen henkilöstö on koulutettu WHO:n periaatteiden mukaisesti ja sen tiedot kulkevat WHO:n verkostojen kautta. Järjestelmä rakennetaan nimenomaan niin, että vastaus on ei.
RAHOITUSKYSYMYS
WHO:n omissa Polaris II -materiaaleissa on yksi yksityiskohta, joka ansaitsee enemmän huomiota kuin se on saanut. WHO:n Länsi-Tyynenmeren alueen erikoisartikkelissa, joka käsittelee tätä harjoitusta, on haudattuna lause, jossa myönnetään, että GHEC-aloitteen mukaista työtä rahoittavat Gatesin säätiö ja Institute of Philanthropy. (22) Tämä ei ole mikään merkityksetön alaviite. GHEC on koko pandemian torjunta-arkkitehtuurin toiminnallinen selkäranka: pysyvä työvoimakehys, jota Polaris käyttää, jota pandemiasopimus vahvistaa ja joka aktivoituu todellisissa epidemioissa.
Pandemiasopimuksen yhteydessä lyhenne GHEC tarkoittaa Global Health Emergency Corps, eli suomeksi suunnilleen maailmanlaajuinen terveyshätätilanneryhmä tai globaali terveyskriisiverkosto.
Merkittävän osan tämän arkkitehtuurin suunnittelusta ja toteutuksesta on rahoittanut yksi yksityinen säätiö.
Tähän voi suhtautua kahdella tavalla. Ensimmäinen reaktio, jonka suuri osa valtamediasta omaksuu, on, että yksityinen hyväntekeväisyysrahoitus maailmanlaajuisen terveydenhuollon hyväksi on pitkäaikainen käytäntö, että Gatesin säätiö on tehnyt aitoa hyvää rokotusten ja tautien hävittämisen saralla, ja että tämän esiintuominen on ensimmäinen askel kohti salaliittoteoriaa. Toinen reaktio on, että maailmanlaajuinen hätätilanteisiin reagointijärjestelmä, jolla on sopimustason oikeudellinen tuki ja joka toimii osittain yhden yksityisen säätiön rahoittamien ja muokkaamien periaatteiden mukaisesti, herättää perusteltuja kysymyksiä demokraattisesta vastuusta, joilla ei ole mitään tekemistä salaliittoteorioiden kanssa.
Molemmat reaktiot voivat olla totta samanaikaisesti. Gatesin säätiön panokset globaaliin terveyteen ovat todellisia. Samoin on totta, ettei mikään äänestäjäkunta missään ole äänestänyt Bill Gatesia seuraavan pandemian institutionaalisten vastatoimenpiteiden suunnittelijaksi. Perustuslaillisessa järjestelmässä, jossa otetaan vastuu vakavasti, väite ”tällä yksityisellä toimijalla on hyvät aikomukset ja hyödylliset resurssit” ei ole riittävä vastaus kysymykseen ”kuka tämä henkilö on ja millä valtuuksilla hän osallistuu tämän suunnitteluun”.
MITÄ POLARIS II TODELLISUUDESSA TESTASI
Kun tarkastellaan toiminnan yksityiskohtia tarkasti, seuraukset tulevat esiin.
Bruneissa kansallisen tautien torjuntakeskuksen (CDC) tapahtumienhallintaryhmä testasi lentokenttiin liittyviä seuranta- ja pikatoimenpidemalleja, ja tarkasteli sen jälkeen rajat ylittävien matkustajien seurantaa naapurimaiden kanssa. (23) Malesiassa kriisivalmius- ja reagointikeskus testasi kansallisen tapahtumanhallintajärjestelmän aktivointia ja koordinoi sitä ASEAN-kumppaneiden kanssa. (24) Harjoituksen aikana kumppaniorganisaatiot osallistuivat ”globaaliin kumppanikartoitustutkimukseen, jota käytettiin reaaliajassa harjoituksen aikana simuloimaan maiden kiireellisten tarpeiden sovittamista käytettävissä oleviin kumppanikapasiteetteihin”. (25)
Tässä harjoitetaan muutakin kuin lääketieteellistä reagointia. Kyse on integroidusta, rajat ylittävästä ihmisten liikkumisen seurannasta, kansallisten tarpeiden ja kansainvälisten kumppanien kapasiteetin reaaliaikaisesta yhteensovittamisesta, standardoidusta tapahtumahallinnan aktivoinnista radikaalisti erilaisissa poliittisissa järjestelmissä ja tekoälytyökalujen käytöstä hätätyövoiman kohdentamiseen. Nämä ovat hallintovalmiuksia. Niiden soveltamisala ulottuu huomattavasti bakteeritautien puhkeamista pitemmälle. Harjoitus perustui kuvitteelliseen bakteeriin. Harjoiteltavat valmiudet eivät ole sidoksissa tiettyyn skenaarioon.
REHELLINEN PUOLUSTUS JA MIKSI SE EPÄONNISTUU
Kaiken tämän rehellinen puolustus menee karkeasti ottaen näin: COVID-19 tappoi miljoonia ihmisiä ja paljasti katastrofaalisia puutteita kansainvälisessä koordinoinnissa. Valvonta oli pirstaloitunutta, rokotteita hamstrattiin, tieto virtasi epätasaisesti, köyhät maat kärsivät pahiten, eikä kukaan ollut vastuussa. Nykyinen arkkitehtuuri on yritys korjata juuri nämä puutteet. Harjoitukset ovat vakiintunut käytäntö. Sopimukset ovat kansainvälisen yhteistyön perusta. 7-1-7-mittarit ovat kohtuullisia suorituskyvyn vertailuarvoja. Koko järjestelmä on jo kauan ollut uudistamisen tarpeessa.
Tässä argumentissa on todellista painoarvoa, ja vakavasti otettavan konservatiivisen tai libertaarisen kriitikon tulisi myöntää se. COVID-toimet olivat katastrofaaliset. Kansainvälinen koordinointi oli huonoa. Halukkuus korjata tilanne ei ole pahantahtoista.
Mutta konservatiivien ja libertaarien vastaväite ei ole se, etteikö mitään pitäisi tehdä. Se on kaksitahoinen.
Ensinnäkin COVID-19:n opetuksista on erimielisyyttä, ja rakenteilla oleva arkkitehtuuri heijastaa vain yhtä näkemystä. Monet vakavasti otettavat analyytikot päättelivät, että koronaviruksen torjunta epäonnistui liian suuren keskitetyn vallan vuoksi, joka toimi puutteellisen tiedon perusteella, ei liian pienen. Ennennäkemättömän ankarat sulkutoimet, koulujen sulkemiset, rokotusvaatimukset, laboratoriovuotohypoteeseja koskevan toisinajattelun tukahduttaminen, luonnollisen immuniteetin väheksyminen ja varhaisen hoidon keskustelujen politisointi – nämä olivat keskitetyn vallan epäonnistumisia, eivät hajautetun hallinnon. Aito jälkiarviointi punnitsisi molemmat epäonnistumisen suunnat. WHO:n arkkitehtuuria rakennetaan lähes yksinomaan ”enemmän koordinaatiota” -oppien pohjalta eikä juuri lainkaan ”vähemmän ylilyöntejä” -oppien ympärille.
Toiseksi rakentamisen nopeus ja laajuus ylittävät kaikki tavanomaiset demokraattiset arviointiprosessit. Kolme vuotta GHEC:n käynnistyksestä sitovaan sopimukseen, yhdenmukaistettuun kansalliseen kehykseen, institutionalisoituun harjoitusohjelmaan ja kahteen maailmanlaajuiseen harjoitukseen. Yksikään kansallinen lainsäädäntöelin ei keskustellut vakavasti seurauksista. Missään vaaleissa tämä ei ollut ratkaiseva tekijä. Pandemiasopimus hyväksyttiin yksimielisesti Maailman terveyskokouksessa, jossa 11 äänesti tyhjää eikä vastalauseita lausuttu, mikä kuulostaa ylivoimaiselta yksimielisyydeltä, kunnes muistaa, että useimpien jäsenvaltioiden väestöillä ei ole aavistustakaan, että mitään tällaista on tapahtunut.
MITÄ KANNATTAA SEURATA
PABS-liitteestä neuvotellaan vuoden 2026 aikana, ja se menee 79. Maailman terveyskokoukseen (26). Kun pandemiasopimus on hyväksytty, se avautuu allekirjoitettavaksi ja ratifioitavaksi. 60 ratifioinnin jälkeen se tulee voimaan. (6)
Kansallisilla parlamenteilla on perustuslaillinen hetki, kun ratifiointi saapuu niiden ovelle. Useimmissa maissa tämä saa vain vähän mediahuomiota, ja ratifiointia pidetään teknisenä muodollisuutena. Toisissa maissa (ja Yhdysvallat on näistä tärkein) ratifiointi kiistetään poliittisesti, eikä sitä välttämättä tapahdu ollenkaan. Yhdysvaltojen kanta nykyisen hallinnon aikana WHO-asioissa yleensä ja pandemiasopimuksen osalta erityisesti tulee olemaan yksi merkittävimmistä tekijöistä, jotka vaikuttavat siihen, tuleeko tästä arkkitehtuurista yleisesti hyväksytty malli vai järjestelmä, josta jotkut suuret maat päättävät jäädä pois.
Toistaiseksi rakenne on valmis. Polaris II osoitti toimivuutensa. HorizonX takaa, että sitä harjoitetaan ja kehitetään edelleen. Sopimuskerros odottaa lopullisia ratifiointeja.
Rehellinen yhteenveto on tämä: vuosina 2023–2026 WHO ja sen kumppanit rakensivat kaikkien silmien alla ja jokaisessa vaiheessa kattavien lehdistötiedotteiden saattelemana nelitasoisen maailmanlaajuisen pandemianhallintajärjestelmän, joka on kattavampi ja toiminnallisesti yhtenäisempi kuin mikään aiemmin olemassa ollut järjestelmä. Pitäisikö tätä pitää kauan odotettuna edistysaskeleena vai hiljaisena ylilyöntinä, riippuu siitä, mitä mieltä olet keskitetystä vallasta, teknokraattisesta hallinnosta ja edellisen pandemian opetuksista.
Mutta arkkitehtuuri on todellinen. Se ei ole salaliitto. Se on projekti. Ja projekti on suurelta osin valmis.
Kirjallisuus
1. World Health Organization Western Pacific. “Countries showcase global health emergency response and coordination capacities through a WHO-led multi-country simulation.” April 2026. https://www.who.int/westernpacific/newsroom/feature-stories/item/countries-showcase-global-health-emergency-response-and-coordination-capacities-through-a-who-led-multi-country-simulation
2. World Health Organization. “Practicing today for tomorrow’s emergencies – WHO convenes countries and partners to simulate response to major disease outbreak.” 27 April 2026. https://www.who.int/news/item/27-04-2026-practicing-today-for-tomorrow-s-emergencies-who-convenes-countries-and-partners-to-simulate-response-to-major-disease-outbreak
3. UN News. “Nations adopt historic pledge to guard against future pandemics.” 21 May 2025. https://news.un.org/en/story/2025/05/1163451
4. Global Biodefense. “What the WHO Pandemic Agreement and IHR Reforms Mean for the Future of Pandemic Preparedness.” 23 July 2025. https://globalbiodefense.com/2025/07/23/what-the-who-pandemic-agreement-and-ihr-reforms-mean-for-the-future-of-pandemic-preparedness/
5. UN News, “Nations adopt historic pledge to guard against future pandemics,” 21 May 2025.
6. World Health Organization. “WHO Pandemic Agreement.” https://www.who.int/health-topics/who-pandemic-agreement
7. World Health Organization. “Stronger together — milestones that mattered in 2025.” 23 December 2025. https://www.who.int/news-room/spotlight/stronger-together-milestones-that-mattered-in-2025
8. World Health Organization. “Global Health Emergency Corps Framework.” Publication B/78043. https://www.who.int/publications/b/78043
9. International Association of National Public Health Institutes. “WHO Global Health Emergency Corps Framework” (PDF). https://ianphi.org/_includes/documents/sections/tools-resources/ghec-highlights/who-ghec-framework.pdf
10. World Health Organization. “WHO and partners activate Global Health Emergency Corps for the first time in response to mpox outbreak.” 29 October 2024. https://www.who.int/news/item/29-10-2024-who-and-partners-activate-global-health-emergency-corps-for-the-first-time-in-response-to-mpox-outbreak
11. World Health Organization. “National Health Emergency Alert and Response Framework.” Publication 9789240113893. 23 October 2025. https://www.who.int/publications/i/item/9789240113893
12. World Health Organization. “WHO launches new country guidance for health emergency coordination.” 23 October 2025. https://www.who.int/news/item/23-10-2025-who-launches-new-country-guidance-for-health-emergency-coordination
13. WHO, “WHO launches new country guidance for health emergency coordination,” 23 October 2025.
14. World Health Organization. “WHO launches new Horizon X Programme for One Health emergency preparedness.” 13 October 2024. https://www.who.int/news/item/13-10-2024-who-launches-new-horizon-x-programme-for-one-health-emergency-preparedness
15. WHO, “Stronger together — milestones that mattered in 2025,” 23 December 2025.
16. WHO, “Practicing today for tomorrow’s emergencies,” 27 April 2026.
17. World Health Organization. “WHO brings countries together to test collective pandemic response.” 4 April 2025. https://www.who.int/news/item/04-04-2025-who-brings-countries-together-to-test-collective-pandemic-response
18. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
19. WHO, “Practicing today for tomorrow’s emergencies,” 27 April 2026.
20. “Sovereignty, equity, solidarity: progress on the Global Health Emergency Corps.” National Library of Medicine, PMC12374631. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12374631/
21. UK House of Commons Library. “What is the proposed WHO Pandemic Preparedness Treaty?” Research Briefing CBP-9550. https://commonslibrary.parliament.uk/research-briefings/cbp-9550/
22. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
23. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
24. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
25. WHO Western Pacific, “Countries showcase global health emergency response and coordination capacities,” April 2026.
Alkuperäinen teksti

In three years, the WHO has assembled a four-layer pandemic governance system. Polaris II was the dress rehearsal.
| Dr. Robert W. Malone May 6 |
While the political class spent the last three years arguing about whether the World Health Organization was secretly trying to take over the world, the WHO did something far more interesting and far more consequential: it built, in plain sight, a complete architecture for managing the next pandemic. And then it ran a dress rehearsal.
The dress rehearsal had a name: Exercise Polaris II. It took place on April 22 and 23, 2026. Twenty-six countries participated, along with 600 health emergency experts and over 25 partner organizations. The scenario was a fictional novel bacterium that had spread across 27 countries and been declared a Public Health Emergency of International Concern.1 Countries activated their emergency coordination structures, mobilized workforces, aligned policies across borders, and (this is worth pausing on) explored AI-enabled tools for workforce planning.2
If you only read the press release, this looks like a tabletop exercise. A drill. A useful one, even, given that the last pandemic killed millions and exposed real coordination failures. Who could object to practice?
But Polaris II is not a standalone event. It is the visible surface of something much larger that has been assembled, piece by piece, since 2023. And once you see the structure, the structure is hard to unsee.
Four Layers, Three Years
What has actually been built is a tightly interlocking, four-layer system that has matured at remarkable speed:
Layer 1: The Treaty Layer. On May 20, 2025, the 78th World Health Assembly adopted the WHO Pandemic Agreement by a vote of 124 in favor, zero against, and 11 abstentions.3 It is only the second legally binding treaty ever negotiated under Article 19 of the WHO Constitution.4 The first was the 2003 Framework Convention on Tobacco Control, and most people have never heard of it because tobacco is unpopular and the treaty was uncontroversial. This one is different. The Pandemic Agreement establishes a Pathogen Access and Benefit Sharing system, a Global Supply Chain and Logistics Network, and a new financial mechanism.5 It enters into force 30 days after 60 ratifications, pending completion of the PABS annex now being negotiated through 2026.6
Sitting alongside the treaty are the 2024 amendments to the International Health Regulations, which came into force in September 2025. Among other changes, they introduced a new “pandemic emergency” alert level, a tier above the existing Public Health Emergency of International Concern designation.7 The IHR has been binding on member states since 2005. The amendments expand its operational reach.
Layer 2: The Framework Layer. The Global Health Emergency Corps was launched at the May 2023 World Health Assembly.8 Its own framework document describes it as “more than a workforce framework; it is a commitment to global solidarity, prioritizing sovereignty and equity.”9 In practice, it is a standing global network of national emergency workforces with mechanisms for surge deployment across borders. It was first activated in October 2024 in response to the mpox outbreak in the Democratic Republic of the Congo.10
In October 2025, the WHO published the National Health Emergency Alert and Response Framework.11 This document tells countries how to structure their domestic emergency response: detection, notification, risk assessment, activation, intervention, review. It embeds the 7-1-7 performance benchmark: seven days to detect an outbreak, one day to notify authorities, seven days to complete early response actions.12 It integrates more than 300 recommendations drawn from COVID-19 reviews into a single national doctrine.13
Layer 3: The Program Layer. HorizonX is the umbrella program that turns simulation exercises from one-off events into a permanent, recurring test regime. It was launched in October 2024 as a multi-year initiative for “multi-sectoral emergency zoonotic disease preparedness.”14 Polaris is just one strand. The WHO ran approximately 50 simulation exercises in 2025 alone.15 The phrase used in WHO’s own materials is telling: preparedness is meant to become “a continuous investment” rather than “a periodic effort.”16
Layer 4: The Exercise Layer. Polaris I in April 2025, with 15+ countries.17 Polaris II in April 2026, with 26.1 Future iterations planned indefinitely under HorizonX. Each exercise stress-tests the layers above it and generates an after-action report that feeds back into framework refinement.18
This is not an accident of bureaucracy. It is a designed system. Each layer reinforces the next. The treaty provides legal authority. The frameworks provide operational doctrine. The program institutionalizes practice. The exercises generate the empirical justification for further build-out.
What the WHO Says About It
The WHO is not secretive about any of this. The Director-General said it plainly after Polaris II concluded: “Exercise Polaris II showed what is possible when we act together. It demonstrated that global cooperation is not optional; it is essential.”19
Read that sentence again. Not optional.
That is not the language of voluntary international coordination among sovereign equals. It is the language of moral obligation backed by institutional architecture. The Director-General is saying (correctly, from his perspective) that the WHO has spent three years building a system in which non-cooperation is no longer a serious option for any country that wants to remain inside the global health order.
A peer-reviewed article in the National Library of Medicine database makes the connection between layers explicit. The Pandemic Agreement, it notes, “reinforces the importance of the GHEC by emphasising that each country should ‘develop, strengthen, and protect a skilled and adequate workforce to prevent, prepare for, and respond to health emergencies, including during pandemics.’” The article continues: “GHEC, with its mandate for rapid response and global health expertise, serves as an operational arm of the Accord. It translates the high-level commitments of the Accord into action.”20
There is no ambiguity here. The framework is the operational arm of the treaty. The exercise tests the framework. The program makes the testing permanent. The treaty makes the whole thing legally durable.
The Sovereignty Question, Honestly Stated
The standard establishment response to concerns about this architecture is to point at specific clauses and say: see, the treaty preserves sovereignty. The text explicitly states it does not authorize the WHO to direct, order, or alter national laws. UK ministers have stated that under no circumstances will the WHO have power to mandate lockdowns.21 WHO spokespeople dismiss the sovereignty concern as misinformation.
These statements are technically accurate. They are also somewhat beside the point.
Sovereignty in the modern administrative state is rarely surrendered by a single dramatic act. It erodes through the accumulation of soft commitments, technical standards, performance benchmarks, peer pressure, funding conditions, and informational dependencies. A country that has signed the Pandemic Agreement, restructured its national emergency workforce per GHEC guidance, adopted the National Alert and Response Framework’s 7-1-7 timelines, integrated its surveillance with the Global Outbreak Alert and Response Network, and committed to participate in HorizonX exercises has not formally surrendered any sovereignty. It has merely made dozens of practical choices that, in aggregate, mean its pandemic response will be functionally indistinguishable from what the WHO would have prescribed.
This is not a conspiracy. It is the normal mechanism by which international technocratic systems operate. The European Union works this way. The IMF works this way. The OECD works this way. What is novel is the speed and scope of the WHO version, and the fact that it is being built specifically around emergency powers, a domain where domestic publics historically grant enormous deference to whoever is identified as the legitimate authority.
When the next pathogen emerges, the question will not be whether national governments retain the legal right to chart their own course. They will. The question will be whether any government, in the heat of an emergency, with its own institutions plugged into WHO frameworks, with its workforce trained on WHO doctrine, with its data flowing through WHO networks, will find it politically possible to deviate. The architecture is being built precisely so the answer is no.
The Funding Question
There is one detail in the WHO’s own Polaris II materials that deserves more attention than it has received. Buried in the WHO Western Pacific feature story on the exercise is a sentence acknowledging that work under the GHEC Initiative is funded by the Gates Foundation and the Institute of Philanthropy.22 This is not a minor footnote. The GHEC is the operational backbone of the entire pandemic response architecture: the standing workforce framework that Polaris exercises, that the Pandemic Agreement reinforces, and that gets activated in real outbreaks. A significant portion of that architecture’s design and implementation has been underwritten by a single private foundation.
Now, you can have two reactions to this. The first reaction, which much of the establishment press takes, is that private philanthropic funding for global health is a longstanding practice, that the Gates Foundation has done genuine good in vaccination and disease eradication, and that pointing this out is the first move in a conspiracy theory. The second reaction is that a global emergency response architecture, with treaty-level legal backing, that operates according to doctrines partly funded and shaped by a single private foundation, raises legitimate questions about democratic accountability that have nothing to do with conspiracy theories.
Both reactions can be true at once. The Gates Foundation’s contributions to global health are real. So is the fact that no electorate anywhere voted for Bill Gates to be a co-architect of the institutional response to the next pandemic. In a constitutional system that takes accountability seriously, “this private actor has good intentions and useful resources” is not a sufficient answer to “who is this person and by what authority does he co-design this.”
What Polaris II Actually Tested
Look closely at the operational details and the implications come into focus.
In Brunei, the Incident Management Team within the national CDC tested airport-linked surveillance and rapid response procedures, then reviewed cross-border traveler monitoring with neighboring countries.23 In Malaysia, the Crisis Preparedness and Response Centre tested activation of the national Incident Management System and coordinated with ASEAN partners.24 Across the exercise, partner organizations contributed to a “global partner mapping survey used in real time during the exercise to simulate the matching of country surge needs with available partner capacity.”25
What is being practiced here is not just medical response. It is integrated, cross-border surveillance of human movement; real-time matching of national needs to international partner capacity; standardized incident management activation across radically different political systems; and the use of AI tools to allocate emergency workforce. These are governance capabilities. They have applications well beyond bacterial outbreaks.
The exercise was framed as a fictional bacterium. The capabilities being rehearsed are agnostic to scenario.
The Honest Defense, and Why It Falls Short
The honest defense of all this goes roughly as follows: COVID-19 killed millions of people and exposed catastrophic failures in international coordination. Surveillance was fragmented, vaccines were hoarded, information flowed unevenly, poor countries got the worst of it, and nobody was in charge. The current architecture is an attempt to fix exactly those failures. Practice exercises are standard. Treaties are how international cooperation works. The 7-1-7 metrics are reasonable performance benchmarks. The whole thing is overdue.
There is real force to this argument, and a serious conservative or libertarian critic should acknowledge it. The COVID response was a disaster. International coordination was bad. The instinct to fix it is not malign.
But the conservative and libertarian objection is not that nothing should be done. It is twofold.
First, the lessons of COVID-19 are contested, and the architecture being built reflects only one set of conclusions. Many serious analysts concluded that the COVID response failed because of too much centralized authority acting on incomplete information, not too little. Lockdowns of unprecedented severity, school closures, vaccine mandates, the suppression of dissent on lab-leak hypotheses, the discrediting of natural immunity, the politicization of early treatment debates; these were failures of centralized authority, not of decentralization. A genuine after-action would weigh both directions of failure. The WHO architecture is being built almost exclusively around the “more coordination” lesson and almost not at all around the “less overreach” lesson.
Second, the speed and scope of the buildout outpace any normal democratic process for evaluating it. Three years from launch of GHEC to a binding treaty, an aligned national framework, an institutionalized exercise program, and two global drills. No national legislature seriously debated the implications. No election anywhere turned on this. The Pandemic Agreement was adopted by consensus at the World Health Assembly with 11 abstentions and no objections, which sounds like overwhelming consensus until you remember that most member state populations have no idea any of this happened.
What to Watch
The PABS annex is being negotiated through 2026 and goes to the 79th World Health Assembly.26 Once adopted, the Pandemic Agreement opens for signature and ratification. After 60 ratifications, it enters into force.6
National parliaments will have a constitutional moment when ratification arrives at their door. In most countries this will receive minimal media attention, and ratification will be treated as a technical formality. In others (and the United States is the most important of these), ratification will be politically contested and may not happen at all. The U.S. position under the current administration on WHO matters generally, and on the Pandemic Agreement specifically, will be one of the more consequential variables in whether this architecture becomes the universal default or a regime that some major countries opt out of.
For now, the structure is built. Polaris II proved it works. HorizonX guarantees it will keep being practiced and refined. The treaty layer is awaiting its final ratifications.
The honest summary is this: between 2023 and 2026, in front of everyone, with full press releases at every stage, the WHO and its partners assembled a four-layer global pandemic governance system more comprehensive and more operationally integrated than anything that has existed before. Whether you think this is overdue progress or quiet overreach depends on what you believe about centralized authority, technocratic governance, and the lessons of the last pandemic.
But the architecture is real. It is not a conspiracy. It is a project. And the project is largely complete.